We are probably all familiar with anxiety that has a clear object or focus. It might be the job interview coming up, the test results coming back, or the difficult conversation that needs to happen. We might not enjoy these kinds of uncertainty, but we can usually hold them, more or less. We know the shape of the worry, and we know it has an end point.
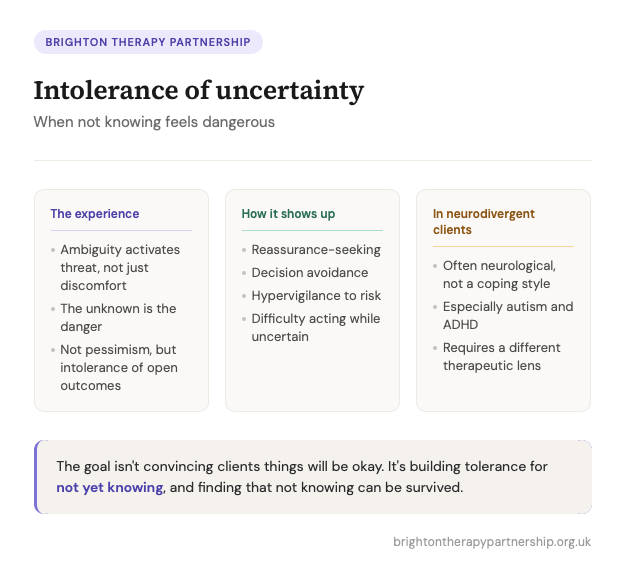
For some people, though, uncertainty itself is a debilitating problem. It may not be about a specific thing and it might be hard to name it, but the simple fact of not knowing, of any kind, about anything. That state of not-yet-resolved is experienced not as uncomfortable, but as genuinely threatening.
This is what we mean when we talk about intolerance of uncertainty. I’m just going to shorten it to IU for the purposes of this article.

It is a concept that has attracted significant research attention over the past two decades, particularly in relation to generalised anxiety disorder, OCD, and health anxiety. But it shows up across a much wider clinical picture than those diagnostic categories.
What intolerance of uncertainty actually is
Intolerance of uncertainty is not pessimism. Clients with high IU do not necessarily expect bad things to happen. What they cannot tolerate is the period of not yet knowing whether something will be okay or not. The research distinguishes between two forms: prospective IU, which is about the future being open and unresolved, and inhibitory IU, which shows up as an inability to function or move forward when things are uncertain. Many clients experience both, but they can present quite differently.
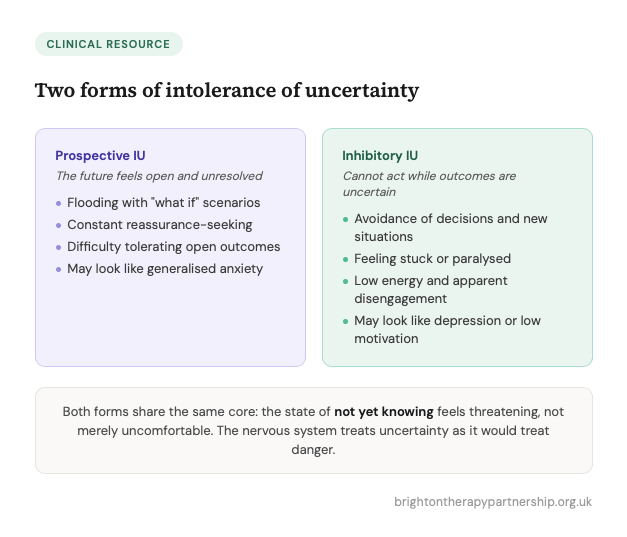 A client with high prospective IU might flood the therapeutic space with “what if” scenarios, not because they think catastrophe is likely, but because generating possibilities feels like a way of closing the gap between now and knowing. A client with high inhibitory IU might present as stuck, avoidant, or lacking in energy in ways that look like depression or low motivation, when what is underneath is an inability to act while outcomes remain unresolved.
A client with high prospective IU might flood the therapeutic space with “what if” scenarios, not because they think catastrophe is likely, but because generating possibilities feels like a way of closing the gap between now and knowing. A client with high inhibitory IU might present as stuck, avoidant, or lacking in energy in ways that look like depression or low motivation, when what is underneath is an inability to act while outcomes remain unresolved.
It is worth naming, with clients and in our own clinical thinking, that this is not a character flaw or a failure of resilience. For many people, a high intolerance of uncertainty developed for entirely good reasons in their personal history. Unpredictable environments, inconsistent caregiving, early experiences of things going badly wrong without warning, these are among the conditions in which IU takes root.
The nervous system learns that uncertainty signals danger. Over time that learning becomes a default.
The neurodivergent dimension
This is particularly relevant when we are working with neurodivergent clients, and it is a dimension that still does not always get enough clinical attention.
For many autistic people, intolerance of uncertainty is not primarily a learned psychological response. It appears to be a core feature of how the nervous system processes information. Autistic neurology often involves a strong preference for predictability, pattern, and sameness that is not about rigidity in any pejorative sense, but about how the brain manages sensory and cognitive load. When that predictability is removed or disrupted, the impact is not just emotional but physiological. Uncertainty taxes the system in a way it simply does not for neurotypical people.
 For people with ADHD, the picture is somewhat different but overlapping. Difficulties with executive function mean that navigating open-ended or ambiguous situations requires considerably more cognitive resources. The anxiety that accompanies uncertainty in ADHD is often compounded by past experiences of things going wrong precisely because of difficulties with planning, organising, or following through, creating a learned association between “I don’t know what happens next” and “things will probably go badly.”
For people with ADHD, the picture is somewhat different but overlapping. Difficulties with executive function mean that navigating open-ended or ambiguous situations requires considerably more cognitive resources. The anxiety that accompanies uncertainty in ADHD is often compounded by past experiences of things going wrong precisely because of difficulties with planning, organising, or following through, creating a learned association between “I don’t know what happens next” and “things will probably go badly.”
Understanding this distinction matters therapeutically. When a neurodivergent client presents with what looks like anxiety driven by IU, the goal is rarely to challenge the perception that uncertainty is dangerous, because that framing may not be accurate to their experience. The work is more likely to involve building genuine support structures, reducing unnecessary ambiguity in the environment, increasing predictability where possible, and helping the client develop a more compassionate relationship with their own nervous system rather than treating their response as a problem to overcome.
How IU shows up in therapy
Across both neurotypical and neurodivergent presentations, intolerance of uncertainty tends to produce recognisable patterns, both in the therapy room and outside. Reassurance-seeking is one of the most common, and one of the trickiest to navigate therapeutically, because reassurance temporarily reduces distress and therefore reinforces the idea that certainty is both obtainable and necessary. The more reassurance a client seeks and receives, the more intolerant of uncertainty they tend to become.

Avoidance is another significant pattern. Clients may avoid making decisions, starting new projects, going to new places, or entering relationships precisely because these things involve outcomes that cannot be known in advance. The avoidance maintains a fragile sense of safety while steadily narrowing the world.
Hypervigilance to threat is a third common feature. Clients with high IU often scan constantly for early signals that something might go wrong, interpreting ambiguous information as evidence of danger. This can look like catastrophising, but the driver is not the catastrophic thought itself, it is the underlying intolerance of not knowing.
What helps
Therapeutic approaches with a good evidence base for IU include cognitive approaches that target the belief that uncertainty is catastrophic or unmanageable, but the how of this matters. Simply challenging “what if” thoughts rarely touches IU at depth. More useful is work that helps clients gradually discover, through experience rather than argument, that uncertainty can be survived, that not knowing does not mean catastrophe is inevitable, and that it is possible to act and engage with life without having certainty in advance.
Exposure-based approaches adapted for IU, sometimes called uncertainty exposure or uncertainty behavioural experiments, ask clients to engage with small doses of deliberate uncertainty and notice what actually happens. This is slow work, and it requires a strong therapeutic alliance. It also requires careful pacing, particularly with neurodivergent clients, where flooding a system that is already taxed is likely to entrench avoidance rather than reduce it.

From a psychodynamic perspective, the relational texture of the therapy itself offers something important. A therapist who can sit with uncertainty in the room, who does not rush to fill silences or provide answers, who can tolerate not knowing alongside the client, provides a form of co-regulation. Over time, this repeated experience of uncertainty being survivable, and of a relationship remaining stable through it, begins to shift something at a deeper level than cognitive restructuring alone can reach.
This is not easy work. But it is, for many clients, some of the most meaningful work there is.
Further reading and resources
Books
Treating Generalized Anxiety Disorder by Michel Dugas and Melisa Robichaud (2007, Guilford Press). This is the foundational clinical text from the researchers who developed the IU model. It is written for practitioners and is clear, structured, and very usable. Worth having on the shelf if you work regularly with anxiety.
The Worry Workbook by Melisa Robichaud and Kristin Buhr (2018, New Harbinger). A client-facing companion to the above, the first self-help workbook to target intolerance of uncertainty directly rather than worry as a general symptom. Useful to recommend to clients, or to draw from therapeutically.
At the time of writing there isn’t yet a single widely-used book specifically on IU written for a general therapeutic readership in the way some other models have spawned, but the two above cover the ground well between them.
For the neurodivergent dimension
Jacqui Rodgers and colleagues at Newcastle University have been among the most active researchers on intolerance of uncertainty in autistic adults, and their work is accessible and clinically grounded. Searching their names alongside “intolerance of uncertainty autism” will bring up several readable papers. The ACAMH website (acamh.org) also has a useful collection of research summaries on IU and neurodevelopmental conditions, written to be accessible rather than purely academic.

Jacqui Rodgers is Professor of Psychology Mental Health and an autism researcher based in the Faculty of Medical Sciences, Newcastle University, UK.
Podcast
Hidden Brain, “Sitting with Uncertainty” (September 2024). Host Shankar Vedantam and psychologist Dannagal Young explore how individual differences in tolerance for ambiguity shape the way people respond to uncertainty, including why some people are drawn to simple explanations when things feel unresolved. Not a clinical episode, but a genuinely interesting listen that many clients would also enjoy. Available on all major podcast platforms.
Join our Therapy Community on Facebook
Brighton Therapy Partnership has a private Facebook Group for therapists which might be of interest to you if you are on social media? We currently have over 2,4k members. You will need to answer all 3 Joining Questions and agree to the Group Rules to join the Group!
Click Here to Join *The Therapy Partnership* Facebook Group – Be Part of the Therapy Community.
Latest Courses

Working with Disordered Eating & Eating Disorders
Explore the emotional and psychological roots of disordered eating and gain essential therapeutic skills to help clients develop a healthier relationship with food, with Prof. Julia Buckroyd. Friday 2nd October…

Healing Traumatic Memory: Essential Skills
This workshop takes a healing-centred, non-narrative approach to trauma, drawing on Somatic Experiencing, EMDR, and IFS to support affect regulation and help clients restore safety and wholeness. With Tracy Jarvis.…
Intrusive Thoughts: A Treatment Guide
Deepen your understanding and therapeutic approach to intrusive thoughts across OCD, anxiety and trauma, transforming your confidence and clinical skills in supporting clients. Saturday 28th November 2026. ONLINE CPD Training…
Get 20% off your first workshop
Join the BTP mailing list and receive a 20% discount code for your first booking — plus early access to new events, blogs & articles, CPD resources, and insights from our expert trainers, straight to your inbox. No spam. Unsubscribe any time.
Therapy Education Online
ThEO is part of Brighton Therapy Partnership
Many of Brighton Therapy Partnership's live events are uploaded to our online library, Therapy Education Online (ThEO).
Therapy Education Online brings the very best of counselling and psychotherapy training to a global audience.
See the full library of training courses through the link below.
Get 20% off your first workshop
Join the BTP mailing list and receive a 20% discount code for your first booking — plus early access to new events, blogs & articles, CPD resources, and insights from our expert trainers, straight to your inbox. No spam. Unsubscribe any time.
Therapy Education Online
ThEO is part of Brighton Therapy Partnership
Many of Brighton Therapy Partnership's live events are uploaded to our online library, Therapy Education Online (ThEO).
Therapy Education Online brings the very best of counselling and psychotherapy training to a global audience.
See the full library of training courses through the link below.
Before submitting, please take note of our community guidelines.